Volume 8, Issue 4 (Journal of Clinical and Basic Research (JCBR) 2024)
jcbr 2024, 8(4): 17-18 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nancy A, Raveendra R, Mohan Sumathi D. Entrapment of neurovascular structures in the (R) popliteal fossa by the third head of the gastrocnemius. jcbr 2024; 8 (4) :17-18
URL: http://jcbr.goums.ac.ir/article-1-441-en.html
URL: http://jcbr.goums.ac.ir/article-1-441-en.html



1- Arunai Medical College and Hospital, Velu Nagar, Thenmathur, Tiruvannamalai - 606603 , ancyjean2010@gmail.com
2- Autonomous State Medical College, Gonda, Uttar Pradesh, India
3- Arunai Medical College and Hospital, Velu Nagar, Thenmathur, Tiruvannamalai – 606603
2- Autonomous State Medical College, Gonda, Uttar Pradesh, India
3- Arunai Medical College and Hospital, Velu Nagar, Thenmathur, Tiruvannamalai – 606603
Full-Text [PDF 342 kb]
(704 Downloads)
| Abstract (HTML) (1372 Views)
Discussion
The first report of an extra head of the gastrocnemius was made in the early 1800s, but the incidence rate and documentation of such cases remain minimal and rare. The origin of the third head of the gastrocnemius has been observed in various regions, including the linea aspera of the femur, as a slip of muscle from the long head of the biceps femoris, the lateral femoral epicondyles, and it may even arise from the knee joint capsule or the fascia of the leg.
In our present case report, the origin of the third head of the gastrocnemius is along with the plantaris muscle and the popliteal surface of the femur, which has been noted as the common type of third head of gastrocnemius (4,5). A similar origin of the third head has also been recorded in cadaveric studies conducted with the same demographic details (5,6). These cadaveric findings have also been substantiated in many radiological studies, where MRI has shown the presence of the third head of the gastrocnemius (4,7).
Our present case report also demonstrated the entrapment of the popliteal artery and the tibial nerve between the medial head and the third head of the gastrocnemius. Studies on popliteal artery entrapment syndrome, which classify the embryological basis of the popliteal artery, categorize the present case of popliteal artery entrapment as type 3. This classification signifies the entrapment of the artery between the medial head of the gastrocnemius and the additional head (4,8).
Not all cases of a third head of the gastrocnemius involve entrapment of the popliteal artery. Some cases of popliteal entrapment syndrome occur with normal anatomy but present with symptoms due to stress maneuvers, and these cases are termed "functional entrapment." A clinical case report described a young male patient who experienced claudication pain, followed by relief in the right leg after continuous walking. MR imaging revealed additional slips of the medial head of the gastrocnemius bilaterally, despite the patient having unilateral symptoms, illustrating the possibility of bilateral involvement (9).
In our report, along with the popliteal artery, the popliteal vein was also noted between the heads of the gastrocnemius, which could be involved in variations of the venous drainage system of the lower limb (10).
Our present report also described a variation in the nerves of the popliteal fossa, where the sciatic nerve exhibits a very low division into the tibial and common peroneal nerves. Additionally, the common peroneal nerve does not wind around the head of the fibula. Similar case reports have recorded bilateral popliteal artery entrapment with normal positioning of the arteries but with the tibial nerve trapped between the heads of the gastrocnemius (11).
Conclusion
Upon reviewing the literature, this study illustrates that an extra head of the gastrocnemius can compress neurovascular structures in the popliteal fossa, potentially causing claudication and limb ischemia. Most commonly, the extra head arises from the medial head of the gastrocnemius. Transection of this extra head can release the entrapped neurovascular structures and relieve symptoms. This condition should be considered in patients presenting with unexplained lower extremity swelling or other symptoms of lower extremity thrombosis.
Acknowledgement
None.
Funding sources
Not Applicable.
Ethical statement
Not Applicable.
Conflicts of interest
The authors declare that they have no competing interests regarding the publication of this article.
Author contributions
AN: Concepts, Design, Data Collection, Manuscript Editing, and Manuscript Review. R: Data Analysis, Manuscript Editing, and Manuscript Review. DMS: Literature Search, Manuscript Preparation, and Manuscript Editing.
Full-Text: (361 Views)
Introduction
The popliteal fossa is an anatomical landmark located behind the knee joint. The arrangement of structures within and around the fossa holds both surgical and pathological significance in humans. Anatomically, the fossa is bounded by the biceps femoris superolaterally and the semitendinosus and semimembranosus superomedially. The inferior boundaries of the fossa are bounded by the two heads of the gastrocnemius. The gastrocnemius is a fusiform-shaped muscle, with medial and lateral heads, considered part of the superficial group of the leg's flexor compartment, along with the soleus and plantaris. Functionally, the gastrocnemius is related to both the knee and ankle joints (1).
Morphologically, there is a difference between the two heads of the gastrocnemius. They arise from the medial and lateral condyles of the femur, with the medial head being larger than the lateral head. Both muscle heads combine to form a common belly. Along with the soleus, they are collectively known as the triceps surae, which attaches to the calcaneum bone (2).
Even though the normal anatomy of the popliteal fossa typically involves the presence of two heads of the gastrocnemius, the incidence of more than two heads is recorded at around 2.9-5.5% (3). This variation can affect the contents of the popliteal fossa, including the popliteal artery, vein, and branches of the sciatic nerve, including tibial and common peroneal nerves. Consequently, this anatomical variation may lead to pathological conditions like popliteal vessel entrapment syndrome and nerve entrapment syndrome, highlighting the need for further knowledge of these variations for surgical and therapeutic management.
Case report
During a routine dissection conducted for teaching undergraduate MBBS students on the lower limb of an approximately 50-year-old male cadaver in the anatomy department, the popliteal fossa was exposed along with the posterior compartment of the thigh and leg on both limbs. The boundaries and contents of the left popliteal fossa appeared normal, but an extra head of the gastrocnemius was found in the right popliteal fossa, running across from the lateral to the medial side (Figure 1). This third head originated from the popliteal surface of the femur near the origin of the plantaris and merged with the medial head of the gastrocnemius, which then joined the lateral head to form the muscle belly. Further exploration revealed a low division of the sciatic nerve, with the popliteal artery, popliteal vein, and tibial nerve (A branch of the sciatic nerve) entrapped between the medial and third heads of the gastrocnemius. Moreover, the common peroneal nerve (Another branch of the sciatic nerve), instead of winding around the neck of the fibula, was sandwiched between the lateral head of the gastrocnemius and the plantaris muscle before subdividing into superficial and deep branches (Figure 2). The cause of death of the cadaver was unknown. However, this anatomical variation is significant, as a literature search revealed few cases of popliteal entrapment syndrome involving either the popliteal blood vessels or the tibial nerve being trapped by an extra head of the gastrocnemius (1-4) or a fibrous band (5,6) connecting the medial and lateral heads. In this case, the neurovascular structures in the popliteal fossa were compressed and trapped between the medial and third heads of the gastrocnemius.
The popliteal fossa is an anatomical landmark located behind the knee joint. The arrangement of structures within and around the fossa holds both surgical and pathological significance in humans. Anatomically, the fossa is bounded by the biceps femoris superolaterally and the semitendinosus and semimembranosus superomedially. The inferior boundaries of the fossa are bounded by the two heads of the gastrocnemius. The gastrocnemius is a fusiform-shaped muscle, with medial and lateral heads, considered part of the superficial group of the leg's flexor compartment, along with the soleus and plantaris. Functionally, the gastrocnemius is related to both the knee and ankle joints (1).
Morphologically, there is a difference between the two heads of the gastrocnemius. They arise from the medial and lateral condyles of the femur, with the medial head being larger than the lateral head. Both muscle heads combine to form a common belly. Along with the soleus, they are collectively known as the triceps surae, which attaches to the calcaneum bone (2).
Even though the normal anatomy of the popliteal fossa typically involves the presence of two heads of the gastrocnemius, the incidence of more than two heads is recorded at around 2.9-5.5% (3). This variation can affect the contents of the popliteal fossa, including the popliteal artery, vein, and branches of the sciatic nerve, including tibial and common peroneal nerves. Consequently, this anatomical variation may lead to pathological conditions like popliteal vessel entrapment syndrome and nerve entrapment syndrome, highlighting the need for further knowledge of these variations for surgical and therapeutic management.
Case report
During a routine dissection conducted for teaching undergraduate MBBS students on the lower limb of an approximately 50-year-old male cadaver in the anatomy department, the popliteal fossa was exposed along with the posterior compartment of the thigh and leg on both limbs. The boundaries and contents of the left popliteal fossa appeared normal, but an extra head of the gastrocnemius was found in the right popliteal fossa, running across from the lateral to the medial side (Figure 1). This third head originated from the popliteal surface of the femur near the origin of the plantaris and merged with the medial head of the gastrocnemius, which then joined the lateral head to form the muscle belly. Further exploration revealed a low division of the sciatic nerve, with the popliteal artery, popliteal vein, and tibial nerve (A branch of the sciatic nerve) entrapped between the medial and third heads of the gastrocnemius. Moreover, the common peroneal nerve (Another branch of the sciatic nerve), instead of winding around the neck of the fibula, was sandwiched between the lateral head of the gastrocnemius and the plantaris muscle before subdividing into superficial and deep branches (Figure 2). The cause of death of the cadaver was unknown. However, this anatomical variation is significant, as a literature search revealed few cases of popliteal entrapment syndrome involving either the popliteal blood vessels or the tibial nerve being trapped by an extra head of the gastrocnemius (1-4) or a fibrous band (5,6) connecting the medial and lateral heads. In this case, the neurovascular structures in the popliteal fossa were compressed and trapped between the medial and third heads of the gastrocnemius.
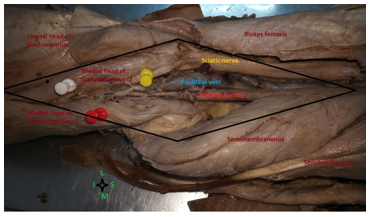 Figure. 1. Right popliteal fossa with boundaries and contents 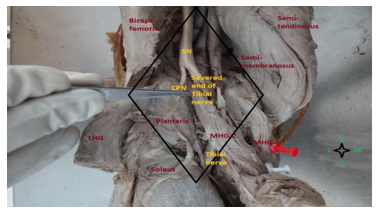 Figure. 2. Entrapment of neurovascular structures in the (R) popliteal fossa SN: Sciatic Nerve, CPN: Common Peroneal Nerve, LHG: Lateral Head of Gastrocnemius, MHG-1: Medial Head of Gastrocnemius, MHG-2: Third Head of Gastrocnemius, S: Superior, I: Inferior, M: Medial, L: Lateral |
Discussion
The first report of an extra head of the gastrocnemius was made in the early 1800s, but the incidence rate and documentation of such cases remain minimal and rare. The origin of the third head of the gastrocnemius has been observed in various regions, including the linea aspera of the femur, as a slip of muscle from the long head of the biceps femoris, the lateral femoral epicondyles, and it may even arise from the knee joint capsule or the fascia of the leg.
In our present case report, the origin of the third head of the gastrocnemius is along with the plantaris muscle and the popliteal surface of the femur, which has been noted as the common type of third head of gastrocnemius (4,5). A similar origin of the third head has also been recorded in cadaveric studies conducted with the same demographic details (5,6). These cadaveric findings have also been substantiated in many radiological studies, where MRI has shown the presence of the third head of the gastrocnemius (4,7).
Our present case report also demonstrated the entrapment of the popliteal artery and the tibial nerve between the medial head and the third head of the gastrocnemius. Studies on popliteal artery entrapment syndrome, which classify the embryological basis of the popliteal artery, categorize the present case of popliteal artery entrapment as type 3. This classification signifies the entrapment of the artery between the medial head of the gastrocnemius and the additional head (4,8).
Not all cases of a third head of the gastrocnemius involve entrapment of the popliteal artery. Some cases of popliteal entrapment syndrome occur with normal anatomy but present with symptoms due to stress maneuvers, and these cases are termed "functional entrapment." A clinical case report described a young male patient who experienced claudication pain, followed by relief in the right leg after continuous walking. MR imaging revealed additional slips of the medial head of the gastrocnemius bilaterally, despite the patient having unilateral symptoms, illustrating the possibility of bilateral involvement (9).
In our report, along with the popliteal artery, the popliteal vein was also noted between the heads of the gastrocnemius, which could be involved in variations of the venous drainage system of the lower limb (10).
Our present report also described a variation in the nerves of the popliteal fossa, where the sciatic nerve exhibits a very low division into the tibial and common peroneal nerves. Additionally, the common peroneal nerve does not wind around the head of the fibula. Similar case reports have recorded bilateral popliteal artery entrapment with normal positioning of the arteries but with the tibial nerve trapped between the heads of the gastrocnemius (11).
Conclusion
Upon reviewing the literature, this study illustrates that an extra head of the gastrocnemius can compress neurovascular structures in the popliteal fossa, potentially causing claudication and limb ischemia. Most commonly, the extra head arises from the medial head of the gastrocnemius. Transection of this extra head can release the entrapped neurovascular structures and relieve symptoms. This condition should be considered in patients presenting with unexplained lower extremity swelling or other symptoms of lower extremity thrombosis.
Acknowledgement
None.
Funding sources
Not Applicable.
Ethical statement
Not Applicable.
Conflicts of interest
The authors declare that they have no competing interests regarding the publication of this article.
Author contributions
AN: Concepts, Design, Data Collection, Manuscript Editing, and Manuscript Review. R: Data Analysis, Manuscript Editing, and Manuscript Review. DMS: Literature Search, Manuscript Preparation, and Manuscript Editing.
Article Type: Case report |
Subject:
Basic medical sciences
References
1. Williams A. Pelvic Girdle and Lower limb. In: Standring S, editor. Gray's Anatomy: The Anatomical basis of clinical practice: 39th edition. Philadelphia:Churchill Livingston Elsevier;1949. [View at Publisher] [Google Scholar]
2. Kaur R, Sharma A, Sharma M. A case report of a variant head of gastrocnemius. Int J Anat Res. 2018;6(3.1):5420-3. [View at Publisher] [DOI] [Google Scholar]
3. Shalini R, Suriyakumari KVP. Third head of gastrocnemius-a case report. National Journal of Clinical Anatomy. 2013;2(3):166-8. [View at Publisher] [DOI] [Google Scholar]
4. Bergman RA, Walker CW, EI-Khour GY. The third head of gastrocnemius in CT images. Ann Anat. 1995;177(3):291-4. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Dave MR, Yagain VK, Anadkat S. Unilateral third/accessory head of the gastrocnemius muscle: A case report. Int J Morphol. 2012;30(3):1061-4. [View at Publisher] [DOI] [Google Scholar]
6. Kumar GR. An anomalous muscle in the region of the popliteal fossa: A case report. J Anat Soc India. 2006;55(2):65-8 [View at Publisher] [Google Scholar]
7. Koplas MC, Grooff P, Piraino D, Recht M. Third head of the gastrocnemius: an MR imaging study based on 1,039 consecutive knee examinations. Skeletal Radiol. 2009;38(4):349-54. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Levien LJ, Veller MG. Popliteal artery entrapment syndrome: more common than previously recognized. J Vasc Surg. 1999;30(4):587-98. [View at Publisher] [DOI] [PMID] [Google Scholar]
9. Tercan F, Oguzkurt L, Kizilkiliç O, Yeniocak A, Gülcan Ö. Popliteal artery entrapment syndrome. Diagn Interv Radiol. 2005;11(4):222-4. [View at Publisher] [PMID] [Google Scholar]
10. Jelev L, Krastev N, Malinova L. An aberrant deep muscle crossing popliteal fossa and concomitant popliteal vein variation. A review of the related muscle and venous variations. Transl Res Anat. 2021;25:100146. [View at Publisher] [DOI] [Google Scholar]
11. Podore PC. Popliteal entrapment syndrome: a report of tibial nerve entrapment. J Vasc Surg. 1985;2(2):335-6. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0).